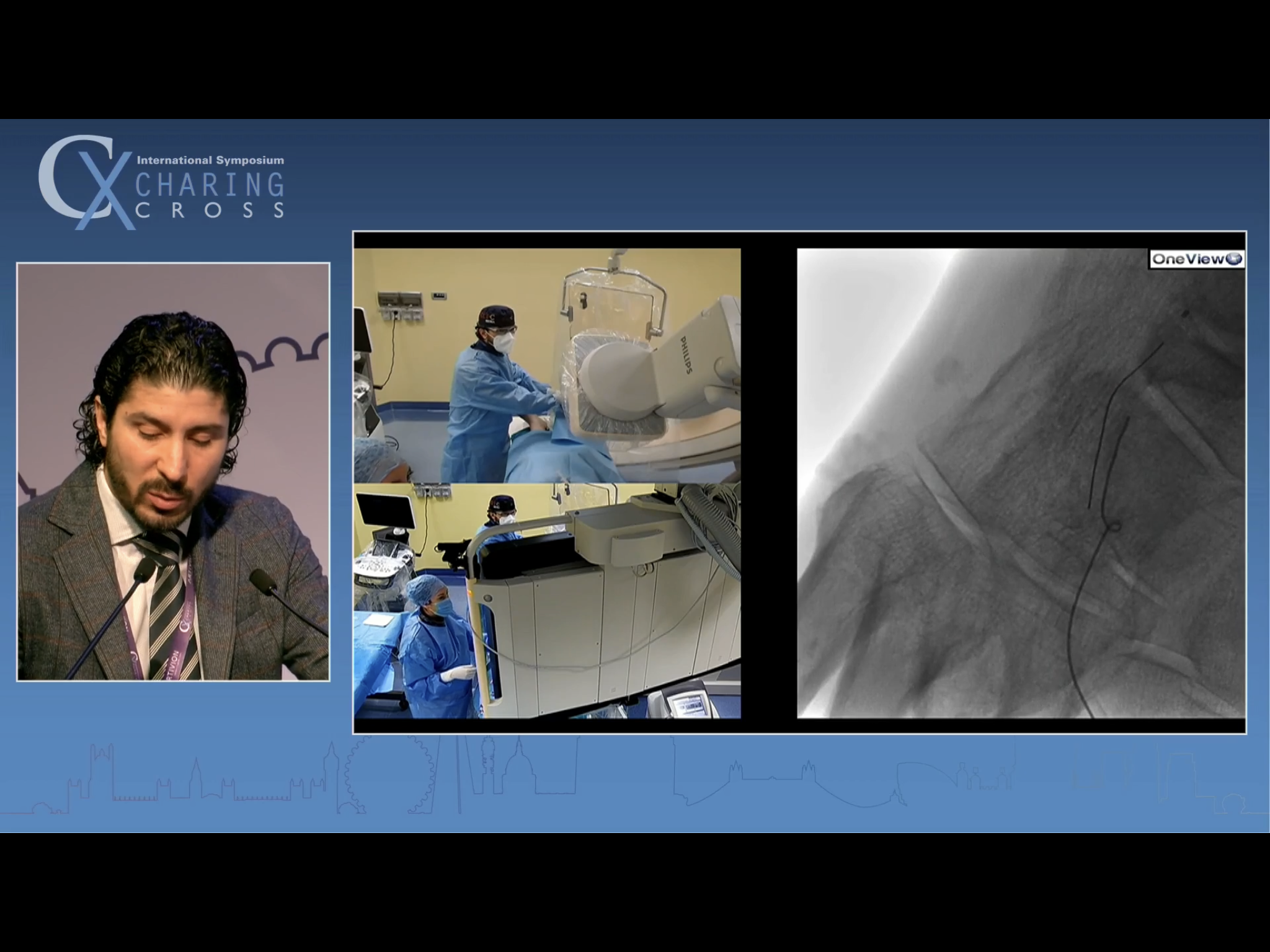
Pedal puncture case - Mariano Palena, Abano Terme
Dr Marco Manzi’s protege presents a talk on CTO technique in very distal BTK CLTI



He says he is using CO2 to minimise contrast load. At the end of the talk he was asked how long these cases take. He said usually 1-2 hours. Said he tries not to go over 2 hours, as he finds that that is when the awake patients lose patience.

The antegrade approach wire is refusing to track down the calcified DPA

Fluoro (and calcium) guided puncture into an arterial branch in the 1st web space

Clearly apparent from the distal (luminal) wire that the retrograde puncture was necessary - the proximal wire has tracked away from the target vessel
manipulation of the retrograde puncture wire into the distal ATA

Capturing the retro wire into the antegrade catheter to achieve through and through access

Retaining the distal wire provides pulsion + traction to get the balloon through into the DPA. He eventually used a 2.5 mm balloon in the DPA. Schneider commented on it. Palena said it was a large vessel.

Having got through, seeking to improve as much of the pedal arch as possible and to get through the loop

I’m afraid I missed capturing the lateral foot run he showed, which looks more impressive than this AP shot.

Ultrasound screening of the Angioseal deployment. I asked if this was standard practice in his unit. He said yes, and said it was a ‘matter of school’. When he started in the unit, Manzi said he could do whatever he wanted, but he must use U/S going in and U/S coming out. So he does.
